
Public health experts warn people to maintain a safe distance in order to disrupt the transmission of Covid-19 – the words we now hear everywhere to refer to this guideline is “social distance”. The more people stay away physically, the more virus transmission will decrease. But the reality is not the same in all contexts, and, as it has been noted by many commentators, households and communities in crowded settings often do not have the conditions to practice social distancing effectively.
How effective can this measure be in Pakistan, a country with a population of 207 million and an average household size of approximately seven members? The situation gets complicated when we realise that approximately 68% of the households have two rooms or less at their disposal. Approximately 50% of the population lives with extended family, which also contributes to a bigger household size. This means that home isolation for Covid-19 patients does not have the desired result and can cause the appearance of family clusters where the virus spreads to other family members in the household.
The disease is expected to take a more dangerous course in densely populated low-income urban areas. In areas where even a neighborhood kiosk or a corner can become a social space for people to congregate in larger groups, social distancing is hard to enforce even in a full lockdown. The majority of the households in these areas also suffer from poor ventilation and inadequate infrastructure and public services, often affecting the levels of hygiene that people are able to maintain.
Even with marked reduction in community contacts, human contact that does not follow social distancing rules is inevitable in such densely and socially connected populations. High population density with intense social networks (upon which people’s livelihoods often depend) provides a favorable condition for increasing disease transmission. Even with strict lockdown rules, transmission within the family is likely to occur.
The household size, population density and social networks’ characteristics have a direct impact on the effectiveness and sustainability of a prolonged lockdown. In countries such as Pakistan where many rely on small business activities and the informal sector for their livelihoods, the negative socio-economic consequences of strict containment measures can be dire.
Pakistan started a full lockdown at the end of March, which then became what government officials called a “smart” lockdown with more targeted testing and tracing, and some commercial and industrial activities allowed to reopen.
With the start of the Islamic holy month of Ramadan, the government also allowed prayer congregations in most parts of the country, giving in to pressure from religious communities. Worshippers should however stay at a minimum of one metre apart from each other, to reduce the chance of contagion.
From 9 May, the lockdown restrictions have been further eased to allow a phased reopening of the economy. Prime Minister Imran Khan urged the public to follow social distancing, and also warned that a new lockdown will be imposed if a rapid increase of cases occurs.
While the economic pressure to reopen is significant, the country needs to strike a delicate balance between the needs of the economy and the health of its citizens.
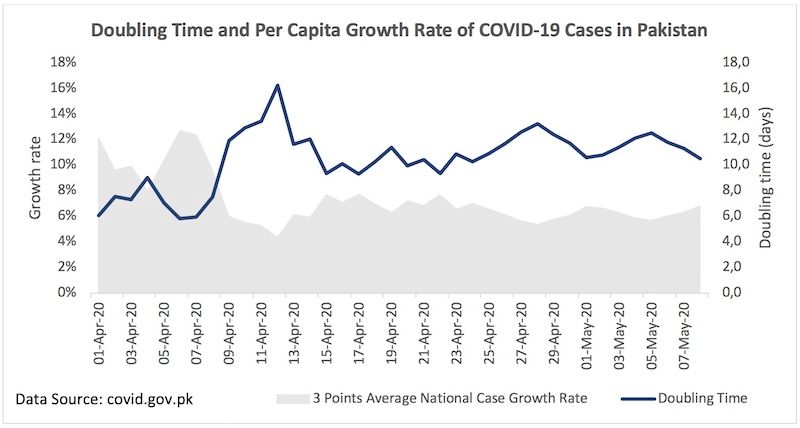
Despite the lockdown, Pakistan’s per capita case growth rate is hovering between 7% and 10%, and the doubling rate (the time it takes for Covid-19 cases to double) is between seven and ten days. The government needs to come up with a sustained strategy to ensure safety while reopening the economy.
If infection control measures are not properly implemented, there is a high risk of an explosion of cases, and of overwhelming the already fragile healthcare system. What Pakistan needs is a multifaceted localised approach to curb the spread of coronavirus.
There are however several challenges on this path. Isolation centres have been set up across the country to avoid the dangers of home isolation, but due to social stigma associated with the disease, not all positive cases are willing to use them.
Testing capacity has also been enhanced since the start of the crisis, reaching at the end of April a daily average of 40 tests per million people. However, the tests were conducted unevenly across the country. Mass testing is not possible at the moment, due to major resource constraints. Despite these obstacles, it is important that testing of all patients with flu-like symptoms in clinics and hospitals continues.
Some provinces are already making progress in this direction by experimenting with pool testing, a strategy to test a larger number of people with less resources.
Multiple samples are taken from a household or a wider area and they are all tested together in one go – which means more swabs are tested at once with the same diagnostic kit, making considerable savings. If the result is a combined negative, there is no need for further tests, as all individuals in that sample are negative. If the pooled sample tests positive, individual tests are carried out to determine who is positive and who is negative.
On the contact tracing front, there is still a lack of efficient and effective mechanisms. Contact tracing needs to be expanded and a network of community volunteers should be trained and deployed as tracers.
These measures should be complemented by sustained and targeted behavioural change campaigns for different segments of the population such as religious leaders, entrepreneurs, industrial workers, academics, and others. This would increase the level of individual compliance with social distancing in the absence of a lockdown.
With a swift and coordinated effort from government and citizens, Pakistan can stave off the threat of public health system collapse, and thus avoid the potentially catastrophic effects of Covid-19. But time is of the essence, and we should all collectively act towards this goal now.
Dr Kamran Baig is an epidemiologist and Associate Director of Monitoring, Evaluation and Research of the Pakistan Country Program of the international NGO Jhpiego, an affiliate of Johns Hopkins University. He has previously managed hospital-based MERS outbreaks in Saudi Arabia.
The views expressed in this article are those of the author and do not necessarily reflect Corona Times’ editorial stance, or the position of any institution or association.